Progesterone Cream: Where to Apply + How to Use
Progesterone Cream: Benefits, How to Use & Where to Apply — 2026 Guide
By Asmae | Women’s Wellness Writer & Hormonal Health Specialist at WellnessSparkles.com
⚠️ This article is for informational purposes only and does not replace professional medical advice. If you are experiencing severe hormonal symptoms, please consult a qualified healthcare provider.
Progesterone cream delivers bioidentical progesterone directly through the skin, bypassing the liver and providing steady hormonal support for symptoms like PMS, heavy periods, insomnia, and perimenopausal hot flashes — with results typically appearing within 8 to 12 weeks of consistent use. How well it works depends on the type of cream you use (over-the-counter vs. compounded prescription), where you apply it, and whether you are testing your levels with the right method. Use the application guide, dosing table, and FAQ below for your specific situation.
Table of Contents
- Progesterone Cream: Benefits, How to Use & Where to Apply — 2026 Guide
- What is progesterone cream and how does it work in your body?
- What are the proven benefits of progesterone cream for women?
- Where should you apply progesterone cream for best absorption?
- How do you use progesterone cream — dosing, timing, and cycle phase?
- Why does progesterone cream not show up on standard blood tests?
- What are the real signs of low progesterone in women — and how does cream address each one?
- What is the cortisol connection — and why are women in their thirties low in progesterone?
- What foods support progesterone cream’s effectiveness?
- Natural supplements that work alongside progesterone cream
- FAQ
- Works Cited
Quick Facts — Progesterone Cream (2026)
| Women Affected by Hormonal Imbalance | Perimenopause Onset Age | Time to See Results | Tissue Absorption vs. Blood Serum |
|---|---|---|---|
| Up to 80% during their lifetime | Ages 45–47 (average) | 8–12 weeks of consistent use | Tissue levels 10–100x higher than serum |
What is progesterone cream and how does it work in your body?
Progesterone cream is a transdermal hormone delivery system that absorbs directly through the skin into the dermal capillary network and lymphatic system, bypassing first-pass liver metabolism entirely. Because progesterone is a fat-soluble molecule, it binds to red blood cell membranes and travels directly to peripheral tissues and cellular receptors, producing measurable hormonal activity without significantly raising standard venous blood levels.
This is the mechanism most mainstream articles completely ignore — and it is the reason so many women are told their cream “isn’t working” when it absolutely is.
When progesterone is absorbed transdermally, it avoids the liver converting it into heavily sedating metabolites, which is exactly what happens with oral progesterone (Prometrium). This makes the cream an excellent option for women who find oral micronized progesterone too drowsy to take during the day. The hormone then binds to intracellular progesterone receptors (PR-A and PR-B) inside target cells, triggers structural changes in those receptors, and initiates a cascade of gene expression changes that take approximately 30 to 60 minutes to produce their initial biological effects. The full genomic impact — meaning changes in mood, cycle regularity, sleep architecture, and uterine lining — accumulates over two to three menstrual cycles of consistent use.
For women with low progesterone caused by anovulation, luteal phase defects, or the cortisol-driven pregnenolone steal, the cream replenishes the hormone that the ovaries or adrenal glands are failing to produce adequately. The result is a rebalancing of the estrogen-to-progesterone ratio, which directly addresses symptoms of estrogen dominance — the heavy periods, breast tenderness, bloating, anxiety, and insomnia that dominate the experience of low progesterone.
What are the proven benefits of progesterone cream for women?
Progesterone cream reduces PMS severity, stabilizes mood by restoring the brain’s allopregnanolone supply, supports the uterine lining to reduce heavy and irregular bleeding, counters estrogen dominance that drives fibroids and breast tenderness, and improves sleep quality by enhancing GABAergic activity — all without the cardiovascular and cancer risks associated with synthetic progestins.
The benefits break down clearly by system:
Neurological Benefits: Progesterone metabolizes into allopregnanolone, a neurosteroid that binds to GABA-A receptors in the brain. When progesterone drops — during the luteal phase, postpartum, or in perimenopause — this GABA support collapses. The result is heightened anxiety, panic attacks, and insomnia. Restoring progesterone through a cream directly rebuilds this neurological buffer. Women with low progesterone who are prescribed SSRIs or benzodiazepines are frequently being treated for a symptom rather than the underlying neurosteroid deficit. Progesterone cream addresses the root cause.
Uterine and Menstrual Benefits: Progesterone transitions the uterine endometrium from an estrogen-driven proliferative state to a mature secretory state. Without adequate progesterone, the lining continues to thicken unopposed, leading to heavy, clotted, and prolonged periods, uterine fibroids, and endometrial hyperplasia. Restoring progesterone halts this proliferation, stabilizes the lining, and normalizes cycle length. Women with luteal phase defects — cycles shorter than 24 days or premenstrual spotting — experience direct improvement in endometrial stability with consistent cream use.
Metabolic and Thyroid Benefits: Progesterone facilitates the cellular action of thyroid hormones and reduces thyroid-binding globulin production in the liver, freeing more active T3 into the bloodstream. This is why so many women with low progesterone present with symptoms that mirror hypothyroidism — fatigue, brain fog, weight gain, cold intolerance — yet their TSH results return within the “normal” range. Restoring progesterone resolves these downstream metabolic disruptions without requiring thyroid medication.
Bone Protection: Progesterone actively stimulates osteoblasts — the cells responsible for building new bone. Its chronic absence accelerates bone density loss independently of estrogen, making adequate progesterone essential for long-term skeletal health, particularly for women in their late thirties and forties who are decades away from conventional menopause.
Where should you apply progesterone cream for best absorption?
Apply progesterone cream to areas with thin skin, minimal body hair, and dense capillary networks: the inner wrists, inner arms, inner thighs, lower abdomen, and behind the knees. These sites maximize transdermal absorption because the hormone travels the shortest distance from the skin surface to the rich capillary beds beneath.
Rotating application sites is non-negotiable. Because progesterone cream is highly fat-soluble, repeated application to the same skin location causes localized tissue saturation. Once that dermal layer becomes saturated, absorption drops significantly. Rotate between three to five sites daily or weekly to maintain consistent uptake. A practical rotation looks like this: inner wrist on Monday, inner arm on Tuesday, behind the knee on Wednesday, lower abdomen on Thursday, inner thigh on Friday.
Sites to avoid: The face, scalp, and breast tissue. While the breast tissue absorbs progesterone efficiently due to its high fat content, routine application there is not recommended given the sensitivity of breast tissue to hormonal stimulation.
How do you use progesterone cream — dosing, timing, and cycle phase?
| User Profile | Recommended Dose | Timing | Application Phase |
|---|---|---|---|
| Premenopausal (PMS, luteal phase defect) | 20–40 mg/day | Days 14–28 of cycle (after ovulation) | Luteal phase only |
| Perimenopause with irregular cycles | 20–40 mg/day | 25 days on, 5–6 days off | Monthly rotation schedule |
| Post-menopause (with estrogen therapy) | 40–100 mg/day (prescription) | Daily or as prescribed | Continuous or cyclic |
| Short luteal phase / spotting before period | 20 mg/day | From ovulation to onset of period | Luteal phase only |
For premenopausal women, the critical rule is to never apply progesterone cream during the follicular phase (days 1–13). Applying it before ovulation suppresses the LH surge, interferes with follicle development, and actively prevents ovulation — the opposite of the intended outcome. The cream is a luteal phase tool.
Timing your first application: Use a basal body temperature chart, ovulation predictor kit, or a progesterone urine strip (such as those from Proov) to confirm ovulation has occurred. Begin cream application the day after confirmed ovulation and continue until the day your period arrives. If your period does not arrive and you are attempting to conceive, continue the cream until you have confirmed with a pregnancy test whether implantation occurred.
Over-the-counter vs. compounded prescription cream: Over-the-counter creams derived from wild yam are classified as cosmetics by the FDA, which means their active hormone concentrations fluctuate significantly between brands and batches. Compounded prescription creams, mixed by specialized pharmacies to a physician’s specification, provide standardized pharmaceutical-grade dosing — typically 40 to 100 mg per mL — and far more predictable clinical outcomes. If you are using an OTC cream and not experiencing results within three cycles, a prescription-grade compounded formulation is the appropriate next step.

Why does progesterone cream not show up on standard blood tests?
Standard venous blood tests show negligible progesterone levels in women using transdermal creams, not because the cream fails to work, but because serum testing measures only the hormone dissolved in the watery portion of blood — and lipophilic progesterone binds to red blood cell membranes and travels through the lymphatic system, bypassing the venous bloodstream almost entirely.
This is the single most important piece of information in this entire article. Pharmacokinetic research confirms that after topical cream application, capillary blood (from a finger prick) and salivary progesterone levels run 10 to 100 times higher than simultaneous venous serum levels. This is not a measurement error. It reflects the actual tissue saturation occurring in the peripheral cells where progesterone does its work.
If your doctor orders a standard venous progesterone draw while you are using a cream and tells you the cream “isn’t raising your levels,” they are using the wrong test for the delivery method.
The correct testing methods for transdermal progesterone:
- DUTCH test (Dried Urine Test for Comprehensive Hormones): Measures progesterone metabolites in dried urine, reflecting tissue-level hormone load accurately
- Capillary blood spot test: At-home finger-prick collection; measures capillary blood levels that accurately reflect tissue saturation
- Salivary assay: Highly sensitive and reflective of free, bioavailable hormone in peripheral tissues
Tracking without testing: If formal testing is not immediately accessible, the most reliable indicators that your cream is working are: your luteal phase lengthening to 12 to 14 days, premenstrual spotting resolving, sleep quality improving in the second half of your cycle, and anxiety reducing in the week before your period.
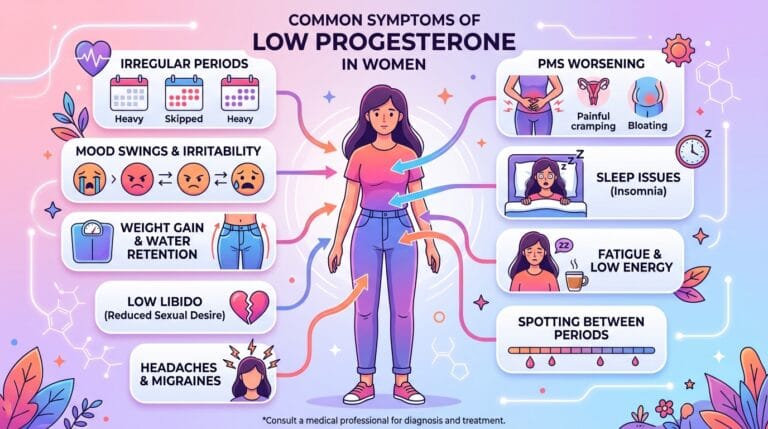
What are the real signs of low progesterone in women — and how does cream address each one?
| Symptom | Underlying Mechanism | How Cream Addresses It |
|---|---|---|
| Anxiety & panic attacks (especially pre-period) | Allopregnanolone deficit collapses GABA-A receptor support | Restores allopregnanolone production, rebuilding natural anxiolytic activity |
| Luteal phase insomnia | Loss of progesterone’s GABAergic sleep-promoting effects | Enhances slow-wave sleep architecture within 2–4 weeks |
| Heavy, clotted periods | Unopposed estrogen drives endometrial hyperplasia | Induces secretory phase, stabilizing and thinning the lining |
| Premenstrual spotting | Premature corpus luteum degradation, insufficient lining support | Extends luteal phase hormonal support, preventing early shedding |
| Short cycles (under 24 days) | Luteal phase defect — progesterone drops too soon | Extends luteal phase to 12–14 days with timed application |
| Breast tenderness | Unopposed estrogen stimulates ductal proliferation | Counters estrogen-driven mammary tissue swelling |
| Brain fog & fatigue | Thyroid hormone action impaired without progesterone support | Frees active T3 by reducing thyroid-binding globulin |
| Fibroids & endometriosis worsening | Estrogen dominance drives tissue growth | Creates hormonal opposition to estrogen-driven proliferation |
What is the cortisol connection — and why are women in their thirties low in progesterone?
In my years working with women on hormonal recovery, the question I hear most often is: “But I’m only 34 — why is my progesterone already low?” The answer is not in the ovaries. It is in the adrenal glands.
Both cortisol and progesterone are synthesized from the same precursor molecule: pregnenolone. Under conditions of chronic psychological or physiological stress, the body hyperactivates the HPA axis and demands continuous cortisol production. To meet that demand, it shunts pregnenolone away from progesterone synthesis and toward cortisol — a process called the pregnenolone steal.
The result is that a 34-year-old woman with a high-pressure career, poor sleep, and chronic low-grade inflammation produces textbook cortisol — and essentially zero meaningful luteal progesterone — despite ovulating regularly. Her blood tests return “normal.” Her doctors find nothing. And she continues experiencing worsening PMS, shorter cycles, anxiety that escalates precisely in the two weeks before her period, and insomnia she cannot explain.
Progesterone cream addresses the downstream deficiency. But to truly resolve the root cause, stress-driven pregnenolone steal requires concurrent HPA axis support: magnesium glycinate at 300 to 400 mg before bed, adaptogenic herbs like ashwagandha, and the dietary interventions detailed below. Women at highest risk are those aged 35 to 45 who endure chronic stress, maintain low-fat diets (which starve steroidogenesis of its cholesterol backbone), or carry a PCOS diagnosis.
What foods support progesterone cream’s effectiveness?
Diet does not replace progesterone cream, but it directly determines whether your body has the biochemical raw materials to produce and utilize progesterone efficiently. Every steroid hormone begins with cholesterol as its backbone. Women eating very low-fat diets are actively starving their steroidogenesis pathway.
Prioritize these foods to support progesterone production:
- Healthy fats: Avocados, extra virgin olive oil, coconut oil, wild salmon, and mackerel provide the lipid infrastructure for pregnenolone and progesterone synthesis
- Zinc-rich foods: Pumpkin seeds, cashews, almonds, and legumes support corpus luteum development and cellular hormone receptor function
- Vitamin B6 sources: Sweet potatoes, poultry, bananas, and spinach serve as enzymatic co-factors in progesterone biosynthesis and GABA production
- Cruciferous vegetables: Broccoli, Brussels sprouts, kale, and cabbage contain DIM (Diindolylmethane) and indole-3-carbinol, which upregulate liver pathways that clear excess estrogen — directly improving the estrogen-to-progesterone ratio
Foods that work against progesterone:
- High-glycemic refined carbohydrates drive hyperinsulinemia, which triggers anovulation and disrupts the luteal phase — exactly what women with PCOS experience
- Excessive alcohol impairs liver function, slowing estrogen clearance and worsening the estrogen-dominant state that progesterone deficiency creates
Natural supplements that work alongside progesterone cream
| Supplement | Daily Dose | Mechanism | Evidence Level | Caution |
|---|---|---|---|---|
| Vitex agnus-castus (Chasteberry) | 20–40 mg standardized extract | Suppresses prolactin via D2 receptor, boosting LH and corpus luteum progesterone output | Strong — 3 menstrual cycles | Avoid with oral contraceptives or dopamine antagonists |
| Magnesium Glycinate | 300–400 mg at bedtime | Enzymatic co-factor for steroidogenesis; inhibits ACTH to reduce pregnenolone steal | Moderate | High doses of citrate/oxide cause digestive upset; glycinate form preferred |
| Vitamin B6 (Pyridoxine) | 50–100 mg/day | Co-factor for progesterone synthesis; enhances hepatic estrogen clearance | Moderate | Do not exceed 200 mg/day — peripheral neuropathy risk |
| Vitamin C (Ascorbic Acid) | 750–1,000 mg/day | Protects corpus luteum from oxidative damage; enhances progesterone synthesis in luteal phase defects | Preliminary | Very safe; very high doses cause bowel tolerance limits |
| Zinc | 15–30 mg/day | Required for DNA-binding zinc finger structures of steroid hormone receptors | Moderate | Balance with copper for long-term use |

FAQ
Where exactly should I apply progesterone cream on my body?
Apply to the inner wrists, inner arms, inner thighs, lower abdomen, or behind the knees — sites where skin is thin and capillary networks are dense. Rotate between three to five sites daily or weekly. Applying to the same location repeatedly causes localized skin saturation and significantly reduces absorption over time.
How long does it take for progesterone cream to work?
Because progesterone works through genomic mechanisms that alter gene transcription across multiple organ systems, symptom relief requires two to three full menstrual cycles of consistent, correctly timed application — approximately 8 to 12 weeks. Neurological improvements like reduced pre-period anxiety and better sleep architecture appear faster, often within the first cycle, while menstrual cycle changes take longer to stabilize.
My doctor says my blood test shows the cream isn’t working. Is that true?
No. Standard venous blood tests are the wrong measurement tool for transdermal progesterone. Because the cream’s lipophilic hormone bypasses the aqueous venous bloodstream, serum levels show negligible results while tissue saturation — the measure that actually matters — runs 10 to 100 times higher. Request a DUTCH test, capillary blood spot test, or salivary assay to accurately evaluate transdermal progesterone absorption.
Is progesterone cream safe to use if I still have my periods?
Q: Is progesterone cream safe to use if I still have my periods? A: Yes, premenopausal women use progesterone cream regularly for PMS, luteal phase defects, short cycles, and premenstrual spotting. Application is timed strictly to the luteal phase — beginning the day after confirmed ovulation and stopping when the period arrives. Never apply during the follicular phase, as this suppresses the LH surge and interferes with ovulation.
Does progesterone cream cause weight gain?
Progesterone cream does not directly cause fat accumulation. The initial introduction of the hormone activates previously dormant estrogen receptors, which produces temporary water retention and bloating in the first one to two cycles. Long-term, achieving optimal progesterone levels supports weight regulation by improving insulin sensitivity, restoring thyroid hormone conversion, and combating the estrogen dominance that promotes visceral fat storage.
What is the difference between bioidentical progesterone cream and synthetic progestins?
Bioidentical progesterone is molecularly identical to the hormone your body produces, derived from plant sources and synthesized to match human progesterone exactly. Synthetic progestins like medroxyprogesterone acetate (Provera) are chemically altered molecules that bind to progesterone receptors but carry significantly elevated risks of fluid retention, mood depression, and cardiovascular complications — risks confirmed in large-scale Women’s Health Initiative data. Bioidentical progesterone carries none of those profiles.
Can I use progesterone cream without estrogen?
Yes, and for many women — particularly those with estrogen dominance, PCOS, or isolated luteal phase defects — using progesterone without additional estrogen is precisely the correct approach. These women produce sufficient or excessive endogenous estrogen; what they lack is the progesterone to oppose and balance it.
Who should avoid progesterone cream?
Women with an active history of hormone-receptor-positive cancers, undiagnosed abnormal vaginal bleeding, severe active liver disease, or a personal history of deep vein thrombosis require strict medical supervision before using any hormonal preparation, including topical bioidentical progesterone.
Works Cited
- National Institutes of Health. “Female Infertility.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK556033/
- National Institutes of Health. “Physiology, Endocrine Hormones.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK538498/
- PubMed Central. “Insights into Perimenopause: A Survey of Perceptions, Opinions on Treatment, and Potential Approaches.” PMC12014197. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC12014197/
- PubMed. “Treatment of postmenopausal women with topical progesterone creams.” PMID 25196424. URL: https://pubmed.ncbi.nlm.nih.gov/25196424/
- PubMed Central. “Small-Molecule Hormones: Molecular Mechanisms of Action.” PMC3603355. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3603355/
- PubMed Central. “Steroids, Pregnancy and Fetal Development.” PMC6987319. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC6987319/
- PubMed Central. “Adrenal and Thyroid Supplementation Outperforms Nutritional Supplementation — Pregnenolone Steal.” PMC4684134. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4684134/
- PubMed. “Comparison of blood spot, salivary and serum progesterone assays in the normal menstrual cycle.” PMID 3708868. URL: https://pubmed.ncbi.nlm.nih.gov/3708868/
- PubMed Central. “Vitex agnus castus for premenstrual syndrome.” PMC6494412. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC6494412/
- PubMed Central. “Efficacy and Tolerability — Vitex agnus-castus, Pyridoxine, and Magnesium in PMS.” PMC10472015. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC10472015/
- PubMed. “Estrogen and progestin bioactivity of foods, herbs, and spices.” PMID 9492350. URL: https://pubmed.ncbi.nlm.nih.gov/9492350/
- Cleveland Clinic. “Low Progesterone: Causes, Symptoms, Tests & Treatment.” URL: https://my.clevelandclinic.org/health/diseases/24613-low-progesterone
- Mayo Clinic. “Menopause — Diagnosis and Treatment.” URL: https://www.mayoclinic.org/diseases-conditions/menopause/diagnosis-treatment/drc-20353401
- Mayo Clinic. “Progesterone (oral route) — Side Effects & Dosage.” URL: https://www.mayoclinic.org/drugs-supplements/progesterone-oral-route/description/drg-20075298
- FDA / HHS. “HHS Advances Women’s Health, Removes Misleading FDA Warnings on Hormone Replacement Therapy.” URL: https://www.fda.gov/news-events/press-announcements/hhs-advances-womens-health-removes-misleading-fda-warnings-hormone-replacement-therapy
10 Best Herbs to Increase Progesterone Levels Naturally Without Any Medication