Low Progesterone Symptoms Women Always Miss
Low Progesterone: Symptoms, Causes & Natural Ways to Boost It
By Asmae | Women’s Wellness Writer & Hormonal Health Specialist at WellnessSparkles.com
⚠️ Medical Disclaimer: This article is for informational purposes only and does not replace professional medical advice. If you are experiencing severe hormonal symptoms, please consult a qualified healthcare provider.
Low progesterone produces symptoms across three distinct body systems — neurological, reproductive, and metabolic — and these symptoms range from insomnia and anxiety to recurrent miscarriage and cycle irregularity. How severe your experience is depends on whether your levels drop suddenly, chronically, or in relation to your estrogen levels. Use the symptom checklist and tables below to identify where your body is signaling a deficiency and which natural interventions apply to your specific situation.
Table of Contents
- Low Progesterone: Symptoms, Causes & Natural Ways to Boost It
- Quick Facts — Low Progesterone (2026)
- What are the most common signs of low progesterone in women?
- What causes low progesterone in reproductive-age women?
- Does low progesterone affect your sleep and mood?
- How do you test your progesterone levels accurately?
- What foods and supplements actually raise progesterone naturally?
- FAQ
- Works Cited
Quick Facts — Low Progesterone (2026)
| Women with Transient Luteal Defects | PMS Global Prevalence | PMDD Prevalence | Athletes Affected |
|---|---|---|---|
| >30% of regular cycles | 47.8% worldwide | 3–8% of reproductive-age women | Up to 60% in endurance sports |
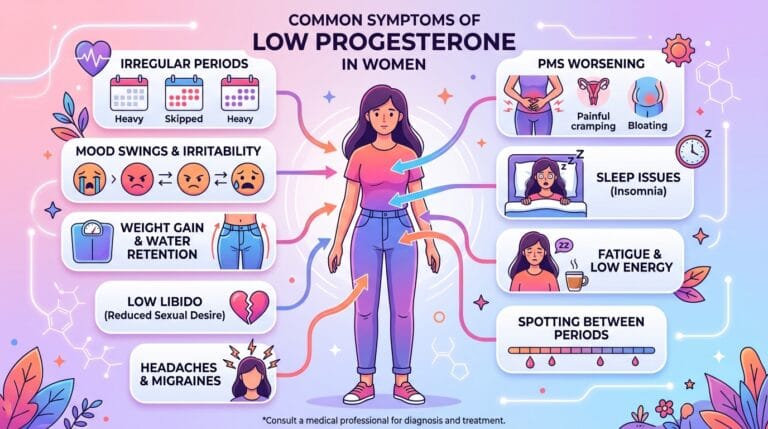
What are the most common signs of low progesterone in women?
Low progesterone produces a recognizable cluster of symptoms that appear in the second half of your cycle — the luteal phase — and resolve within a day or two of your period starting. The core signs are: shortened cycles under 21 days, premenstrual spotting, luteal phase insomnia, severe mood swings or anxiety, breast tenderness, bloating, and worsening migraines in the days before your period.
What makes low progesterone particularly confusing is that these symptoms mimic at least two other common conditions: hypothyroidism and primary depression. The fatigue, weight changes, and sleep disruption are virtually indistinguishable from a sluggish thyroid. The cyclical mood crashes are routinely — and incorrectly — diagnosed as bipolar disorder or major depressive disorder, when the root cause is a drop in allopregnanolone, progesterone’s primary metabolite, which directly activates calming GABA receptors in your brain.
The key distinguishing feature of low progesterone is timing. If your worst symptoms hit like clockwork in the 7–14 days before your period and lift the moment bleeding begins, progesterone deficiency is the most likely culprit — not a primary mood disorder.
Symptom Checklist: Low Progesterone vs. Low Estrogen
| Symptom | Low Progesterone | Low Estrogen |
|---|---|---|
| Insomnia (luteal phase only) | ✅ Primary symptom | Rare |
| Anxiety & mood swings | ✅ Severe in luteal phase | Moderate, unpredictable |
| Breast tenderness (cyclical) | ✅ Premenstrual | Rare |
| Bloating & fluid retention | ✅ Premenstrual | Rare |
| Hot flashes & night sweats | ❌ Not typical | ✅ Primary symptom |
| Vaginal dryness | ❌ Not typical | ✅ Primary symptom |
| Short cycles (<21 days) | ✅ Yes | Possible |
| Heavy, prolonged bleeding | ✅ Unopposed estrogen | Possible |
| Recurrent early miscarriage | ✅ Primary concern | Rare |
| Bone density loss | Rare | ✅ Primary concern |
What causes low progesterone in reproductive-age women?
The single most common cause of low progesterone is anovulation — the complete absence of ovulation. When ovulation does not occur, the corpus luteum, the temporary gland that produces nearly all of your luteal progesterone, never forms. No corpus luteum means progesterone levels remain at near-zero throughout the second half of your cycle.
In women of reproductive age, anovulation is most frequently driven by three upstream triggers: PCOS, chronic stress, and overexercise. In PCOS, chronic hyperinsulinemia disrupts follicle maturation, preventing the LH surge required to trigger ovulation. In chronic stress, elevated cortisol directly suppresses GnRH pulsing from the hypothalamus through what functional medicine practitioners call the pregnenolone steal — your body diverts the shared cholesterol precursor away from progesterone production toward cortisol synthesis, because survival always wins over reproduction. Among endurance athletes and women in high-aesthetics sports, between 21% and 60% experience anovulatory cycles due to low energy availability disrupting the HPO axis.
A second, separate mechanism is true Luteal Phase Deficiency (LPD) — where ovulation does occur, but the resulting corpus luteum is structurally weak. It either produces insufficient peak progesterone or fails prematurely, cutting the luteal phase to 10 days or fewer instead of the standard 14. This is the scenario that drives premenstrual spotting, severe PMS, and implantation failure.
Women in their late 30s entering perimenopause experience a third cause: ovarian aging. The remaining follicles become resistant to FSH and LH, producing erratic ovulation and low-quality corpora lutea. This explains why progesterone drops years before estrogen does in perimenopause, creating a state of relative estrogen dominance with heavy bleeding and severe mood instability long before a woman identifies as “perimenopausal.”
Does low progesterone affect your sleep and mood?
Low progesterone directly triggers insomnia and anxiety through a specific neurochemical pathway most articles never discuss. Progesterone converts in the brain to allopregnanolone, a potent neurosteroid that binds to GABA-A receptors — the same receptors targeted by anti-anxiety medications. When allopregnanolone disappears with the falling corpus luteum in the late luteal phase, GABA signaling collapses, causing nervous system hyperarousal, fragmented sleep architecture, and a spike in anxiety that is pharmacologically indistinguishable from a panic disorder.
In my years working with women navigating hormonal imbalances, the most consistently overlooked symptom of low progesterone is not mood swings or irregular cycles — it is the relentless, 2 AM waking that begins exactly two weeks before the period. These women have often been given sleep medications, antidepressants, or a PMDD diagnosis, when what their brain is missing is the GABA-activating effect of allopregnanolone. Addressing progesterone directly, not masking the downstream symptom, resolves the insomnia within one to two cycles for the majority of women I work with.
This neurochemical mechanism also explains why postpartum depression behaves the way it does. The massive, sudden clearance of progesterone and allopregnanolone within hours of delivery is the largest hormonal drop a woman’s body ever experiences. Research confirms this state produces a clinically significant allopregnanolone withdrawal — not a primary depressive disorder — which is why IV allopregnanolone analogs produce rapid, dramatic relief in clinical settings.
How do you test your progesterone levels accurately?
Standard blood tests for progesterone are accurate only when drawn at exactly the right time — 5 to 7 days after confirmed ovulation. The ubiquitous “Day 21 test” instruction that many doctors still give produces dangerously misleading results in any woman whose cycle is not a textbook 28 days. A woman with a 35-day cycle who ovulates on Day 21 will show near-zero progesterone if tested on Day 21 — she is simply still in her follicular phase, and a misdiagnosis of anovulation follows.
Even perfectly timed blood draws carry a second problem: progesterone is secreted in discrete pulses controlled by LH, and a single blood draw can vary up to eightfold within a 90-minute window. A single reading of 3 ng/mL is technically within conventional “normal” range (1.8–24 ng/mL), but functionally indicates a weak corpus luteum incapable of suppressing PMS or supporting implantation.
Progesterone Levels: Conventional vs. Functional Medicine Standards
| Phase / Situation | Conventional Lab Range | Functional Medicine Optimal | What It Means |
|---|---|---|---|
| Follicular Phase (Days 1–13) | 0.1–0.9 ng/mL | <1.0 ng/mL | Normal; progesterone should be suppressed here |
| Mid-Luteal Phase (5–7 days post-ovulation) | 1.8–24.0 ng/mL | 10–25 ng/mL | Levels of 3–9 ng/mL indicate luteal phase defect |
| Suboptimal Luteal Phase | N/A | 5.0–9.9 ng/mL | Ovulated, but corpus luteum is weak |
| Probable Anovulation | N/A | <5.0 ng/mL (mid-luteal) | Follicle likely did not rupture |
| First Trimester Pregnancy | 11.2–90.0 ng/mL | Minimum >10 ng/mL | Below 10 ng/mL triggers rescue protocol consideration |
For women who want more comprehensive data than a single blood draw provides, at-home urinary monitors measuring Pregnanediol-3-Glucuronide (PdG) — the urinary metabolite of progesterone — are now clinically validated. Systems like Mira, Proov, and Inito measure PdG over several days, mapping the full luteal phase rather than capturing one pulsatile peak or trough. A sustained PdG reading of ≥5 µg/mL across days 7–10 past peak fertility confirms a robust luteal phase with 80–100% specificity.
What foods and supplements actually raise progesterone naturally?
Three nutrients produce the strongest and most evidence-supported impact on progesterone production: Vitamin B6, magnesium, and zinc. These work upstream, supporting the enzymatic steps that convert cholesterol into pregnenolone and progesterone, and protecting the corpus luteum from oxidative degradation.
Vitex agnus-castus (Chaste Tree Berry) is the most studied herb for luteal insufficiency. At standardized doses of 4 mg to 40 mg daily, Vitex acts as a dopaminergic agonist, suppressing prolactin secretion from the pituitary. Elevated prolactin blocks ovulation and impairs corpus luteum function — reducing it restores normal LH pulsing and natural progesterone output. Most women see measurable cycle improvement within 3 menstrual cycles (approximately 90 days).
Women with low progesterone symptoms related to estrogen dominance also benefit from prioritizing cruciferous vegetables — broccoli, cauliflower, and Brussels sprouts — which support the liver’s ability to clear excess estrogen, thereby improving the progesterone-to-estrogen ratio without directly supplementing either hormone. If you are working to flush out excess estrogen through diet, adding ground flaxseed (1 tbsp daily in the follicular phase) and ground sunflower and sesame seeds in the luteal phase constitutes the seed cycling protocol shown in preliminary clinical trials to improve cycle regularity and luteal phase length over 3 to 6 months.
Because all progesterone is synthesized from cholesterol, a low-fat diet actively undermines corpus luteum function. Avocados, fatty cold-water fish, grass-fed butter, and nuts provide the lipid substrates your steroidogenic cells require. Simultaneously, eliminating endocrine-disrupting chemicals from plastics, synthetic fragrances, and conventional food packaging removes xenoestrogens that bind to estrogen receptors and further suppress your progesterone ratio.
For a full breakdown of herbs that directly support luteal function, the article on herbs to increase progesterone covers dosing and evidence levels in detail.
Natural Interventions for Low Progesterone: Evidence Guide
| Intervention | Dose | Evidence Level | Time to Results | Key Caution |
|---|---|---|---|---|
| Vitex agnus-castus | 4–40 mg daily (standardized extract) | Moderate–High | 3 menstrual cycles | Avoid with hormonal contraceptives or IVF protocols |
| Vitamin B6 | 50–100 mg daily | High | 3 cycles | >200 mg/day risks peripheral neuropathy |
| Magnesium Glycinate | 310–320 mg daily | Moderate | 1–2 cycles | Avoid high-dose in kidney disease |
| Zinc (elemental) | 8–30 mg daily | Moderate | 2–3 cycles | Take with food; high doses require copper balance |
| Seed Cycling (Luteal: sunflower + sesame) | 1 tbsp each, daily (Days 15–28) | Preliminary/Moderate | 3–6 months | Not suitable for seed allergies |
| Vitamin E + Selenium | 400 IU E + 200 µg Se | Moderate | 2–3 months | Vitamin E interacts with blood thinners |
| Stress Management (CBT, Yoga, Breathwork) | Daily practice | Strong | 1–3 cycles for hormonal shift | None |
| Sleep Hygiene (7–9 hrs, dark/cool room) | 65–68°F, complete darkness | Strong | 2–4 weeks for CNS adaptation | None |
Understanding how cortisol affects your menstrual cycle is essential if stress is the upstream driver of your low progesterone — because no supplement corrects anovulation caused by an overactive HPA axis unless cortisol is addressed first.
FAQ
What is the fastest way to raise progesterone naturally?
The fastest natural intervention is addressing the upstream cause. If stress-induced anovulation is the driver, 300–320 mg of magnesium glycinate nightly combined with daily breathwork or yoga practice produces measurable improvement in HPA axis regulation within 2 to 4 weeks. Vitex requires 3 menstrual cycles for full corpus luteum remodeling, making magnesium and B6 the faster-acting pair for immediate PMS symptom relief.
Can low progesterone cause anxiety and panic attacks?
Yes. The drop in progesterone during the late luteal phase removes allopregnanolone’s direct activation of GABA-A receptors in the brain, causing nervous system hyperarousal that produces anxiety, panic, and insomnia. This is a neurochemical event, not a psychological one, and it resolves completely at the start of menstruation when the hormonal baseline resets.
How do I know if my cycle is anovulatory?
The clearest signs of an anovulatory cycle are: a luteal phase shorter than 10 days, mid-luteal progesterone below 5 ng/mL, absence of a biphasic temperature shift on basal body temperature tracking, and the disappearance of fertile cervical mucus without a detectable LH surge. At-home monitors measuring PdG across multiple days in the luteal phase confirm or rule out ovulation with 80–100% specificity.
Does low progesterone cause weight gain?
Low progesterone causes fluid retention and cyclical bloating by removing its competitive inhibition of aldosterone. Without adequate progesterone blocking aldosterone receptors, your kidneys retain sodium and water, producing the premenstrual weight increase and puffiness most women experience in the week before their period. This is water retention driven by hormonal imbalance — not fat accumulation — and it resolves within 48 hours of menstruation starting.
Can you have low progesterone with regular periods?
Yes. Ovulation and menstruation are not the same event. A woman produces a period even in anovulatory cycles — estrogen builds the uterine lining, and its eventual withdrawal triggers bleeding regardless of whether a corpus luteum ever formed. A regular 28-day cycle with consistent bleeding provides no confirmation that ovulation occurred or that luteal progesterone was adequate. Only mid-luteal blood testing or PdG monitoring confirms corpus luteum quality.
Is low progesterone connected to recurrent miscarriage?
Luteal phase deficiency is a confirmed contributing factor in recurrent early pregnancy loss. Without adequate progesterone, the endometrium cannot complete the secretory transformation required for blastocyst implantation. Women with a history of recurrent miscarriage who additionally present with early pregnancy bleeding represent a specific subgroup — confirmed in updated ASRM guidelines — who benefit meaningfully from targeted progesterone supplementation, producing improved live birth rates.
Works Cited
- NIH/PubMed. “Menstrual Health in Servicewomen: The Menstrual Cycle, Menstrual Disturbances, and Occupational Consequences.” PMC (2024). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC12770106/
- ASRM. “Diagnosis and Treatment of Luteal Phase Deficiency: A Committee Opinion.” (2021). URL: https://www.asrm.org/practice-guidance/practice-committee-documents/diagnosis-and-treatment-of-luteal-phase-deciency-a-committee-opinion-2021/
- NIH/PubMed. “New Pharmacological Approaches to the Management of Premenstrual Dysphoric Disorder.” PMC (2023). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC10212816/
- NIH/PubMed. “Rising Global Burden of Common Gynecological Diseases in Women of Childbearing Age from 1990 to 2021.” PMC (2024). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC12010537/
- NIH/PubMed. “Mechanisms of Angioregression of the Corpus Luteum.” PMC (2023). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC10568036/
- NIH/PubMed. “Anatomy, Abdomen and Pelvis, Ovary Corpus Luteum.” NCBI Bookshelf (2023). URL: https://www.ncbi.nlm.nih.gov/books/NBK539704/
- NIH/PubMed. “Physiology, Progesterone.” NCBI Bookshelf (2023). URL: https://www.ncbi.nlm.nih.gov/books/NBK558960/
- NIH/PubMed. “Luteal Insufficiency in First Trimester.” PMC (2012). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3659905/
- NIH/PubMed. “The Inadequate Corpus Luteum.” PMC (2022). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC8812462/
- Cleveland Clinic. “Low Progesterone: Causes, Symptoms, Tests & Treatment.” URL: https://my.clevelandclinic.org/health/diseases/24613-low-progesterone
- Cleveland Clinic. “Luteal Phase Defect: Causes, Symptoms & Treatment.” URL: https://my.clevelandclinic.org/health/diseases/luteal-phase-defect
- NIH/PubMed. “Progesterone and Its Metabolites Play a Beneficial Role in Affect Regulation in the Female Brain.” PMC (2023). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC10143192/
- ASRM. “Fertility Evaluation of Infertile Women: A Committee Opinion.” (2021). URL: https://www.asrm.org/practice-guidance/practice-committee-documents/fertility-evaluation-of-infertile-women-a-committee-opinion-2021/
- NIH/PubMed. “Vitex agnus-castus Effects on Hyperprolactinaemia.” PMC (2024). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC11018691/
- NIH/PubMed. “Impact of Nutritional Diet Therapy on Premenstrual Syndrome.” PMC (2023). URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC9928757/
10 Best Herbs to Increase Progesterone Levels Naturally Without Any Medication