Progesterone vs Estrogen: 7 Signs You’re Off Balance
Progesterone vs Estrogen: Key Differences & How to Balance Both
By Asmae | Women’s Wellness Writer & Hormonal Health Specialist at WellnessSparkles.com
⚠️ This article is for informational purposes only and does not replace professional medical advice. If you are experiencing severe hormonal symptoms, please consult a qualified healthcare provider.
Estrogen builds and proliferates — it thickens your uterine lining, drives your monthly cycle, and shapes your female characteristics — while progesterone calms, differentiates, and counterbalances everything estrogen starts. The ratio between the two determines whether your body functions smoothly or spirals into weight gain, insomnia, anxiety, and irregular periods. Use the quick facts box and full breakdown below to understand exactly where your imbalance likely begins.
Quick Facts — Progesterone vs Estrogen (2026)
| Women Affected by Hormonal Imbalance | PCOS Prevalence (Global) | Endometriosis Cases Worldwide | Time for Natural Interventions to Work |
|---|---|---|---|
| 80% experience some form during their lifetime | 6–13% of reproductive-age women | ~190 million women | 8–12 weeks (2–3 full cycles) |
What is the actual difference between progesterone and estrogen?
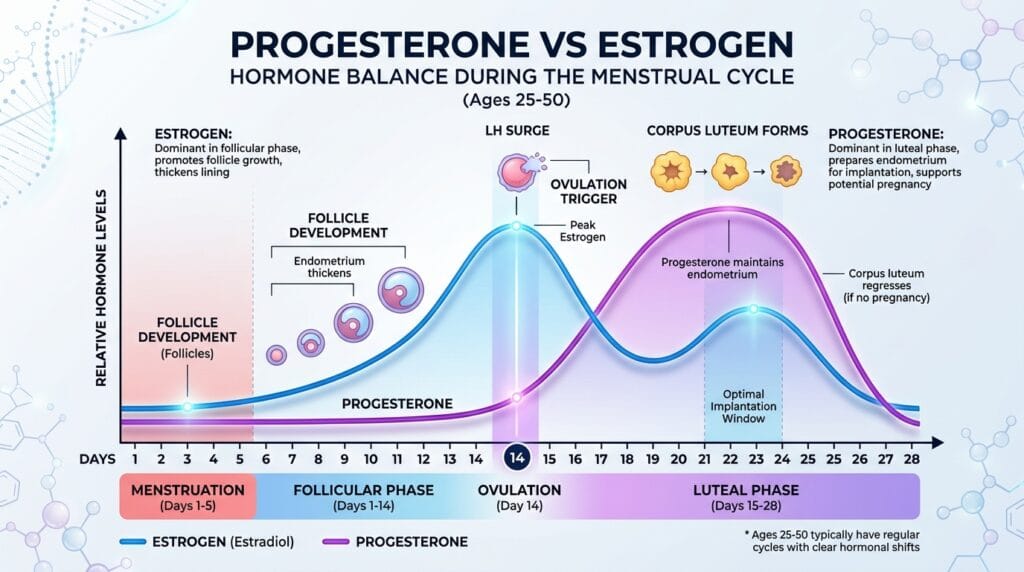
Estrogen drives cellular proliferation throughout the first half of your cycle, building tissue, supporting bone density, and regulating cardiovascular function — while progesterone takes over after ovulation to halt that growth, calm the nervous system, and prepare the uterus for potential pregnancy. These two hormones are not opposites — they are partners in a precise biological rhythm, and when one falls out of step, your entire body registers the disruption.
Your body produces three primary estrogens — estradiol (E2), estrone (E1), and estriol (E3) — with estradiol being the most potent during your reproductive years. Estradiol is manufactured by the granulosa cells of your developing ovarian follicles. It binds to estrogen receptors throughout your brain, bones, cardiovascular system, and reproductive tract, acting as a master metabolic regulator with wide-ranging effects far beyond fertility.
Progesterone, by contrast, is produced almost exclusively after ovulation by the corpus luteum — the temporary gland that forms from the ruptured follicle. In the second half of your cycle (days 15–28), progesterone halts the estrogen-driven thickening of the uterine lining and converts it into secretory tissue ready to receive an embryo. If pregnancy does not occur, the corpus luteum breaks down, progesterone plummets, and menstruation begins.
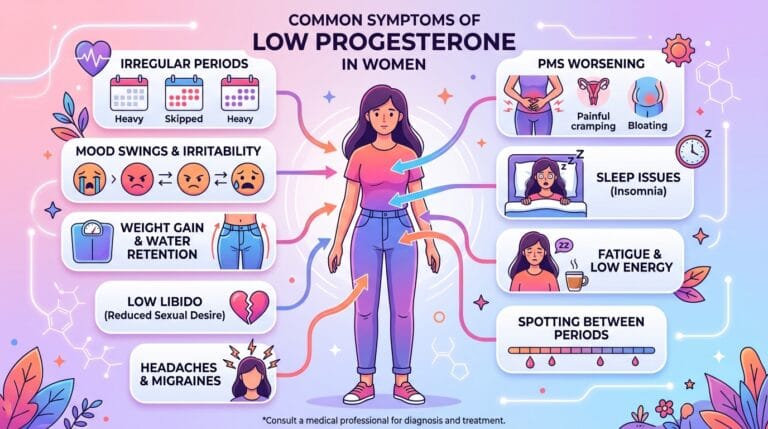
What most articles completely miss: progesterone’s metabolites — specifically allopregnanolone — cross the blood-brain barrier and bind directly to GABA receptors, producing a profound calming, anti-anxiety, sleep-promoting effect. This is why low progesterone shows up not just as period problems, but as relentless insomnia and crushing pre-period anxiety.

What happens when estrogen and progesterone fall out of balance?
Estrogen dominance — the state in which estrogen is disproportionately high relative to progesterone — produces heavy periods, breast tenderness, bloating, weight gain around the hips and abdomen, intense PMS, and mood instability. This imbalance develops even when absolute estrogen levels are not actually elevated, as long as progesterone is absent or critically low.
The most common driver in women aged 25–40 is anovulation. In conditions like PCOS, follicles develop but never rupture. Without ovulation, no corpus luteum forms, which means zero progesterone production while the unruptured follicles continue secreting estrogen. The result is a chronic state of unopposed estrogenic stimulation.
What Most Articles Get Wrong About Perimenopause
Most wellness blogs tell you that menopause is when your hormones drop. This misses the most critical window of hormonal chaos your body experiences. During perimenopause — which frequently begins in your late 30s or early 40s — progesterone levels decline precipitously years before estrogen does. Your aging ovaries skip ovulations increasingly often, meaning the corpus luteum forms less and less frequently. Meanwhile, the remaining follicles respond erratically to FSH signals, causing estradiol to surge wildly to levels sometimes higher than those seen in your 20s. The result is a 5-to-10-year window of severe estrogen dominance before your periods even stop — and this is the window where most women are dismissed, misdiagnosed, and left to suffer without answers.
Symptoms by Hormone Imbalance Type
| Symptom | Points to Low Progesterone | Points to Estrogen Dominance | Points to Low Estrogen |
|---|---|---|---|
| Insomnia (especially luteal phase) | ✓ Primary sign | ✓ Contributing | — |
| Heavy, prolonged periods | ✓ | ✓ Strong indicator | — |
| Breast tenderness / fibrocystic breasts | ✓ | ✓ | — |
| Hot flashes / night sweats | — | ✓ (perimenopausal) | ✓ (postmenopausal) |
| Severe PMS / PMDD | ✓ Primary sign | ✓ | — |
| Bloating / fluid retention | ✓ | ✓ | — |
| Vaginal dryness | — | — | ✓ |
| Anxiety / mood swings | ✓ (GABA disruption) | ✓ | ✓ |
| Bone loss / osteoporosis | ✓ (osteoblast reduction) | — | ✓ (osteoclast activation) |
| Rapid abdominal weight gain | ✓ | ✓ | ✓ |
How does chronic stress destroy your progesterone levels?
Chronic stress causes the adrenal glands to mass-produce cortisol by diverting the biochemical precursor pregnenolone away from progesterone synthesis — a process called the pregnenolone steal — leaving progesterone production critically depleted while estrogen continues unchecked. This is not a theory; it is a well-documented physiological mechanism that guarantees estrogen dominance in chronically stressed women.
Pregnenolone is the master steroid from which your body manufactures both cortisol and progesterone. Under perceived threat — whether from work stress, poor sleep, blood sugar dysregulation, or chronic inflammation — your biology prioritizes immediate survival over reproduction every single time. Cortisol wins. Progesterone crashes. And because this happens quietly, without dramatic symptoms, most women spend years on anti-anxiety medications or antidepressants when the root cause is sitting entirely in their adrenal stress response.
In my years working with women navigating hormonal imbalances, one pattern repeats itself constantly: the woman who comes in convinced she has a thyroid problem — exhausted, gaining weight despite eating well, losing hair, foggy and depressed — whose TSH is completely normal. What is actually happening is that excess estrogen increases hepatic production of Thyroid Binding Globulin (TBG), a protein that binds to free thyroid hormones and renders them biologically inactive. Her thyroid is producing hormones. Her body simply cannot use them because estrogen is blocking delivery. Once we address the root hormonal imbalance, thyroid function normalizes without medication. This cortisol-to-progesterone-to-estrogen cascade is the hidden engine behind a remarkable number of thyroid misdiagnoses.
If you recognize this pattern in yourself, understanding how cortisol affects your menstrual cycle is the essential next step.
What do your hormone lab results actually mean?
Standard laboratory reference ranges flag overt disease, not optimal function — meaning a woman experiencing severe perimenopausal symptoms is routinely told her bloodwork is “normal” because her levels have not yet crossed into a clinically recognized disease state.
Functional medicine uses narrower “optimal” ranges modeled to reflect peak physiological function. The critical distinction: conventional medicine measures individual hormone levels; functional medicine measures the ratio between hormones, which determines whether your cells are experiencing estrogenic dominance regardless of what any single number says. For accurate testing, progesterone and estradiol must be drawn during the mid-luteal phase — typically day 21 of a 28-day cycle, or 7 days after confirmed ovulation.
Conventional vs Functional Lab Ranges (Mid-Luteal Phase)
| Biomarker | Conventional Normal Range | Functional Optimal Range | What Low Levels Mean |
|---|---|---|---|
| Estradiol (E2) | 27–246 pg/mL | 60–120 pg/mL (luteal: 80–180 pg/mL) | Vasomotor symptoms, bone loss, cognitive decline |
| Progesterone (Pg) | 2.6–21.5 ng/mL | 10–20 ng/mL (mid-luteal) | Levels <5 ng/mL confirm anovulation or luteal phase defect |
| Pg/E2 Ratio | Not standardly measured | 100–500 ratio | <100 confirms estrogen dominance; >500 suggests progesterone dominance |
| FSH | Up to 21.5 mIU/mL | 4.0–7.0 mIU/mL | Values >7 indicate diminished ovarian reserve; >30 confirms menopause |
For women in perimenopause, a single blood draw is insufficient — hormones fluctuate so wildly day-to-day that a snapshot result is nearly meaningless. Advanced DUTCH (Dried Urine Test for Comprehensive Hormones) panels map daily circadian hormone output and metabolic breakdown pathways, identifying specifically whether your liver is clearing estrogen into protective metabolites or inflammatory, DNA-damaging forms.
What foods and supplements actively restore hormone balance?
A targeted nutritional protocol directly supports the liver’s capacity to clear excess estrogen, improves insulin sensitivity to prevent anovulatory cycles, and provides the micronutrient cofactors required for corpus luteum health and progesterone production. Diet is not complementary here — it is foundational.
Foods that actively restore balance:
Cruciferous vegetables (broccoli, Brussels sprouts, cauliflower, kale) contain indole-3-carbinol, which converts to DIM in the gut. DIM shifts estrogen metabolism toward protective 2-hydroxyestrone and away from the inflammatory, cancer-promoting 16-hydroxyestrone. Aim for 1–2 cups daily.
Ground flaxseed (1–2 tablespoons daily) provides lignans — phytoestrogens that act as natural SERMs, competitively blocking potent endogenous estradiol at receptor sites while supporting liver clearance. In high-estrogen states they block; in low-estrogen states they provide mild estrogenic support. This is the nuance most blogs miss entirely when they tell you to avoid all phytoestrogens.
High-fiber foods targeting 30g daily bind deactivated estrogen in the intestines and facilitate its excretion. Without adequate fiber, gut bacteria produce an enzyme called beta-glucuronidase that strips deactivated estrogen of its protective bonds, allowing it to be reabsorbed into circulation and dramatically elevating systemic estrogen load.
Foods to eliminate or minimize:
Alcohol places a massive detox burden on the liver, delaying estrogen clearance significantly while simultaneously promoting the aromatization of androgens into estrogens. Refined carbohydrates and sugar drive chronic hyperinsulinemia, which forces the ovaries to produce androgens instead of progesterone — a self-perpetuating cycle of worsening hormonal ratios. Conventional red meat and high-fat dairy contribute synthetic growth hormones and animal-derived estrogens directly to your system. You can explore this further in the complete guide to flushing out excess estrogen.
Natural Supplement Protocol for Hormone Balance
| Supplement | Daily Dose | Mechanism | Time to Results | Key Caution |
|---|---|---|---|---|
| Vitex Agnus-Castus (Chasteberry) | 20–30 mg standardized extract | Binds dopamine D2 receptors in anterior pituitary, reducing prolactin and allowing full corpus luteum development and progesterone production | 8–12 weeks (2–3 cycles) | Avoid with hormonal birth control or IVF drugs; ineffective postmenopause |
| DIM (Diindolylmethane) | 100–200 mg | Optimizes liver Phase I estrogen metabolism toward protective 2-hydroxyestrone metabolites | 4–6 weeks | May initially cause mild headaches as detoxification accelerates; darkens urine |
| Magnesium + Vitamin B6 | 300 mg Mg + 30 mg B6 | Downregulates HPA axis stress response, reducing cortisol to prevent pregnenolone steal; B6 is a cofactor in liver estrogen detoxification | 4–8 weeks | High magnesium citrate doses may cause osmotic diarrhea |
| Black Cohosh | 40–80 mg standardized extract | Acts as a SERM, suppressing pro-inflammatory cytokines and binding serotonergic receptors to reduce vasomotor symptoms without proliferating uterine tissue | 4–8 weeks | Contraindicated with active liver disease or estrogen-receptor-positive breast cancer |
| Ground Flaxseed (Lignans) | 1–2 tablespoons | Phytoestrogenic lignan activity competitively blocks potent estradiol at ER-beta receptors | 8–12 weeks | Must be ground for bioavailability; alters absorption of oral medications if taken simultaneously |
What does the 2025/2026 science actually say about hormone therapy?
Body-identical hormone therapy, initiated before age 60 or within 10 years of menopause onset, produces significant cardiovascular, bone, and cognitive protection — benefits that the 2025 FDA removal of black box HRT warnings confirmed definitively outweigh the previously overstated risks. The outdated 2002 Women’s Health Initiative data — which used synthetic progestins, not body-identical progesterone — drove decades of fear that left millions of women undertreated.
In November 2025, the FDA officially removed broad black box warnings linking HRT to breast cancer and cardiovascular disease. The extended longitudinal analysis that prompted this action confirmed that estrogen monotherapy demonstrates a reduction in breast cancer incidence in specific healthy cohorts. The 2025 European Society of Endocrinology guidelines — endorsed by the Endocrine Society and ACOG — now advocate for early, individualized MHT to prevent irreversible bone demineralization and cardiovascular damage. The UK’s NICE guidelines updated simultaneously to reinforce individualized care and elevate the use of transdermal bioidentical administration.
The key clinical distinction: synthetic progestins (like medroxyprogesterone acetate used in the WHI) carry higher risks than micronized progesterone. Transdermal estradiol — delivered through patches, gels, or sprays — bypasses hepatic first-pass metabolism entirely, eliminating the venous thromboembolism risk previously associated with oral synthetic estrogens. If your doctor is still citing 2002 data to deny you hormone therapy, that guidance is medically outdated.
FAQ
What is the earliest sign that progesterone is low?
The most reliable early sign is a shortened menstrual cycle — particularly a luteal phase lasting fewer than 10 days — combined with spotting that begins 3–5 days before the full period starts. Relentless pre-menstrual insomnia beginning exactly in the second half of your cycle is another definitive indicator. Blood testing on day 21 confirms it: progesterone levels below 5 ng/mL confirm anovulation or a severe luteal phase defect.
Can estrogen dominance cause anxiety and depression?
Yes. Estrogen dominance, combined with progesterone deficiency, results in the failure of allopregnanolone — progesterone’s neurosteroid metabolite — to adequately bind to GABA receptors in the brain. This produces neurological hyper-excitability: racing thoughts, heightened anxiety, emotional volatility, and depressive episodes that are concentrated in the luteal phase. These symptoms are routinely misdiagnosed as generalized anxiety disorder or major depression, leading to inappropriate SSRI prescriptions when the root cause is endocrine.
How long does it take to rebalance hormones naturally?
Natural interventions — dietary changes, targeted herbs like Vitex, and supplements like DIM and magnesium — require a minimum of 2–3 full menstrual cycles (8–12 weeks) to produce measurable physiological changes. Blood tests show objective improvement in that timeframe. Bioidentical hormone replacement therapy produces faster results for severe vasomotor symptoms, often within 2–4 weeks.
Does progesterone make you gain weight or lose weight?
Progesterone promotes the loss of fluid retention by competing with aldosterone at mineralocorticoid receptors, producing a diuretic effect. Adequate progesterone also supports thyroid hormone receptor sensitivity, improving metabolic rate. The weight gain most women associate with progesterone is actually caused by the estrogen dominance that results from progesterone deficiency — not progesterone itself.
Is it safe to take progesterone without estrogen?
Progesterone-only therapy is a well-established, safe approach for women in perimenopause who still produce adequate or fluctuating estrogen but have stopped ovulating regularly. It is also highly effective for PMDD and severe PMS. For postmenopausal women, the clinical decision depends on symptom profile and individual health history — this is where functional lab testing and a practitioner partnership become essential.
What is the Pg/E2 ratio and why does it matter?
The Pg/E2 ratio is calculated from mid-luteal phase blood values and provides the most clinically meaningful single data point for assessing hormonal balance. A functional optimal ratio falls between 100 and 500. A ratio below 100 confirms clinical estrogen dominance — even if both individual values appear “normal” in isolation. Standard lab panels do not calculate this ratio automatically, which is why women are so frequently told they are fine when they are not.
Does stress directly affect my period?
Chronic stress triggers the pregnenolone steal — diverting the precursor steroid pregnenolone away from progesterone synthesis toward cortisol production. The result is direct: reduced progesterone, shortened or skipped luteal phases, irregular cycles, and worsening PMS. This is the physiological link between a demanding job, a difficult life period, or chronic poor sleep and the sudden onset of irregular, painful, or heavy periods.
Works Cited
- NIH — StatPearls. “Physiology, Progesterone.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK558960/
- NIH — StatPearls. “Physiology, Menstrual Cycle.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK500020/
- NIH — StatPearls. “Hormone Replacement Therapy.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK493191/
- NIH — PubMed Central. “Progesterone Actions and Resistance in Gynecological Disorders.” URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC8870180/
- NIH — PubMed Central. “Estrogen: An Emerging Regulator of Insulin Action and Mitochondrial Function.” URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4391691/
Signs of Low Progesterone: 12 You’re Ignoring