Signs of Low Progesterone: 12 You’re Ignoring
Signs of Low Progesterone: 12 You’re Ignoring
By Asmae | Women’s Wellness Writer & Hormonal Health Specialist at WellnessSparkles.com
⚠️ This article is for informational purposes only and does not replace professional medical advice. If you are experiencing severe hormonal symptoms, please consult a qualified healthcare provider.
Signs of low progesterone range from irregular periods and relentless insomnia to severe anxiety and unexplained weight gain — all beginning in the two weeks before your period. How severely these symptoms affect you depends on your age, stress levels, whether you are ovulating, and how far your estrogen-to-progesterone ratio has shifted out of balance. Use the symptom checklist and tables below to identify exactly where your body is sending you signals.
Table of Contents
- Signs of Low Progesterone: 12 You’re Ignoring
- Quick Facts — Low Progesterone (2026)
- What are the most common signs of low progesterone in women?
- Why does low progesterone cause anxiety and insomnia?
- What does low progesterone do to your menstrual cycle?
- Can low progesterone cause weight gain and bloating?
- What are the signs of low progesterone that doctors most often miss?
- How does low progesterone connect to estrogen dominance?
- What natural remedies raise progesterone levels?
- What foods support or harm progesterone levels?
- FAQ
- Works Cited
Quick Facts — Low Progesterone (2026)
| Women with suboptimal luteal progesterone | Cycles lacking ovulation signs | Time for natural interventions to work | Most misdiagnosed as |
|---|---|---|---|
| Up to 31.3% of normal cycles | 47% in a study of 211,000+ cycles | 90 days (3 full cycles) | Anxiety or depression |
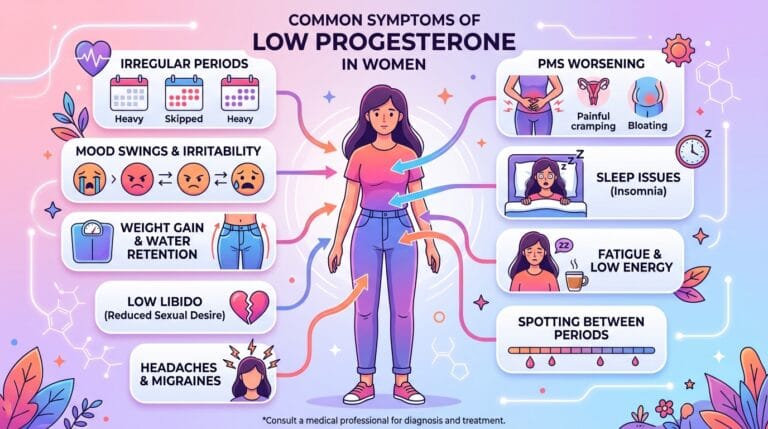
What are the most common signs of low progesterone in women?
The most common signs of low progesterone are premenstrual spotting, shortened cycles under 24 days, sleep disruption in the luteal phase, worsening PMS, breast tenderness, hormonal anxiety, and persistent bloating. These symptoms emerge because the corpus luteum fails to produce enough progesterone to counterbalance estrogen, leaving your body in a state of relative estrogen dominance.
Most women first notice these signs in their late 20s or 30s, often years before any doctor considers testing their hormones. What makes this particularly frustrating is that your cycle may look regular on the surface — but beneath it, your luteal phase is quietly failing. A cycle that appears normal at 28 days can still have deficient progesterone if ovulation was weak or the corpus luteum collapsed too early. Your body is not broken; it is communicating a very specific imbalance.
Your actionable step: Start tracking your cycle phase and note when symptoms appear. If they cluster in the 10–14 days before your period, low progesterone is the first hormonal system to investigate.

Why does low progesterone cause anxiety and insomnia?
Low progesterone causes anxiety and insomnia because the hormone metabolizes into allopregnanolone in the brain — a powerful neurosteroid that activates GABA receptors, the brain’s primary calming system. When progesterone drops, this natural sedative effect disappears, leaving the nervous system hyper-excitable and triggering insomnia, panic, and a “wired-but-tired” restlessness that no amount of chamomile tea resolves.
This is the piece most medical articles completely miss. They list “anxiety” as a checkbox symptom without explaining why your nervous system is misfiring. The reality is biochemical: without adequate progesterone converting into allopregnanolone, your GABA receptors are starved of their natural activator. This is why women with low progesterone frequently describe feeling exhausted but unable to switch off, lying awake at 3 AM with racing thoughts that seem entirely irrational — because they are not rooted in psychology. They are rooted in neurobiology.
In my years working with women experiencing hormonal imbalances, the most consistently overlooked symptom of low progesterone is not anxiety or irregular periods — it is the relentless insomnia that begins precisely in the luteal phase, two weeks before the period. Women are told they have generalized anxiety disorder. They are prescribed SSRIs. Their hormones are never tested. Research confirms that women are twice as likely as men to receive SSRI prescriptions, often masking an underlying hormonal deficit entirely.
Your actionable step: If your insomnia worsens specifically in the week before your period and resolves when menstruation starts, request a mid-luteal serum progesterone test timed 5–7 days after confirmed ovulation — not a generic Day 21 draw.
What does low progesterone do to your menstrual cycle?
Low progesterone shortens the luteal phase to fewer than 10 days, produces cycles under 24 days, and triggers brown spotting before the period starts. It also causes heavy menstrual bleeding because estrogen, unopposed by sufficient progesterone, over-thickens the uterine lining until it sheds excessively.
The premenstrual spotting deserves special attention. That brown discharge appearing 2–5 days before your period is not a quirk or a sign of infection — it is progesterone withdrawing too early, causing the endometrial lining to begin breaking down before true menstruation begins. When progesterone stays elevated long enough, the lining holds stable until the proper hormonal cue. When it collapses prematurely, you spot.
Menstrual Symptom Comparison: Low Progesterone vs. Low Estrogen
| Symptom | Low Progesterone | Low Estrogen |
|---|---|---|
| Cycle length | Short (< 24 days) | Irregular or absent |
| Spotting | Brown spotting before period | Light or no spotting |
| Period flow | Heavy or flooding | Light or scanty |
| PMS severity | Severe, particularly mood | Mild PMS, more physical |
| Breast changes | Tenderness & swelling | Decreased breast fullness |
| Vaginal dryness | Uncommon | Very common |
| Mood pattern | Anxiety, irritability | Low mood, flat affect |
| Hot flashes | Mild, perimenopausal | Frequent and intense |
| Libido | Reduced | Significantly reduced |
Your actionable step: Track your cycle start date, spotting days, and period flow for two cycles. Bring this record to your provider — it gives diagnostic clarity that a single blood draw cannot.
Can low progesterone cause weight gain and bloating?
Low progesterone causes weight gain through two direct mechanisms: it removes the body’s natural diuretic effect, triggering sodium and water retention, and it creates estrogen dominance, which promotes visceral fat accumulation around the abdomen and slows the metabolic rate by impairing thyroid hormone conversion.
Women often describe this weight as different from ordinary gain — it arrives in the week before the period, settles mostly in the belly and breasts, and resists every calorie restriction attempt. That is because it is not a calorie problem. Estrogen dominance drives adipogenesis, particularly visceral fat storage, while low progesterone simultaneously reduces gastrointestinal motility, causing constipation and significant abdominal bloating. Addressing the hormonal root cause of estrogen dominance produces results that dieting alone never achieves.
Your actionable step: Note whether your bloating and weight fluctuate with your cycle. Perimenstrual bloating that resolves within 2–3 days of your period starting is a clear hormonal signal, not a digestive disease.
What are the signs of low progesterone that doctors most often miss?
The most frequently missed signs of low progesterone are brain fog, memory decline, hormonal migraines, recurrent miscarriage, low libido, and bone density loss — symptoms so diverse that they are routinely attributed to separate conditions rather than recognized as a unified hormonal deficiency.
Most wellness articles frame low progesterone as a reproductive or menstrual issue. This misses a fundamental clinical reality: progesterone is a whole-body hormone with receptors in the brain, thyroid, bones, gut, and cardiovascular system. Consider this:
- Brain fog and memory decline result from progesterone’s neuroprotective role. Its absence reduces myelin sheath maintenance in the central nervous system, directly impairing cognitive clarity and memory retrieval.
- Hormonal migraines are triggered by a steep luteal drop in progesterone destabilizing mast cells and triggering inflammatory prostaglandins, causing cerebral vasospasm at the same point each cycle.
- Recurrent early miscarriage results from the endometrium failing to maintain adequate vascularization for implantation, and from insufficient immunomodulation to protect the embryo from maternal immune attack.
- Low libido stems from the combined effect of fatigue, mood disruption, and the depletion of androgen precursor pools that require progesterone as a building block.
- Bone density loss is accelerated because progesterone independently stimulates osteoblast activity — the cells that build new bone. Anovulatory women with chronic deficiency develop osteopenia years earlier than expected.
The misdiagnosis rate is staggering. Women experiencing severe perimenopausal progesterone crashes have been diagnosed with rapid-cycling bipolar disorder. Women with progesterone-induced thyroid sluggishness are treated for primary hypothyroidism. The endocrine evaluation that would clarify everything is simply not ordered.
How does low progesterone connect to estrogen dominance?
Low progesterone produces estrogen dominance even when estrogen levels are completely normal, because progesterone’s job is to counterbalance estrogen’s proliferative effects. Without sufficient progesterone, estrogen drives fibroid growth, endometriosis progression, breast tissue overstimulation, and gallbladder dysfunction — none of which require excess estrogen to occur.
Women with estrogen dominance frequently seek help for what appear to be separate problems: fibroids diagnosed by a gynecologist, anxiety managed by a psychiatrist, insomnia addressed by a sleep specialist. The hormonal thread connecting all three is rarely identified. Correcting the progesterone deficit addresses the root of this entire cascade.
What natural remedies raise progesterone levels?
Natural interventions raise progesterone by supporting the HPG axis, enhancing ovarian follicle quality, providing the enzymatic cofactors required for steroidogenesis, and lowering the cortisol that suppresses ovulation. The most evidence-backed options are Vitex agnus-castus, Vitamin C, Vitamin B6, Magnesium, and Zinc — with clinical improvement appearing after approximately 90 days of consistent use.
A critical correction most articles get wrong: stress does not “steal” progesterone via the pregnenolone steal pathway. Current endocrinological evidence refutes this theory entirely. What stress actually does is elevate cortisol, which signals the hypothalamus to suppress GnRH — shutting down the entire ovulation process. No ovulation means no corpus luteum. No corpus luteum means no progesterone. The production machinery is switched off, not robbed. This distinction matters enormously for treatment: you cannot supplement your way out of a stress-induced ovulation problem without addressing the stress itself. Supporting your adrenal axis through cortisol management is not a lifestyle bonus — it is the prerequisite for hormonal recovery.
Natural Progesterone Support: Evidence-Based Guide
| Supplement | Daily Dose | Evidence Level | Mechanism | Time to Results | Key Caution |
|---|---|---|---|---|---|
| Vitex agnus-castus (Chasteberry) | 20–40 mg (standardized extract) | Strong | Binds dopamine receptors, reduces prolactin, reverses LH suppression, stimulates corpus luteum | 90 days (3 cycles) | Do not combine with OCP, HRT, or dopamine agonists |
| Vitamin C (Ascorbic Acid) | 750 mg | Moderate–Strong | Antioxidant protection for corpus luteum; directly raises serum progesterone in LPD | 1–2 cycles | High doses cause GI upset; caution with kidney stones |
| Vitamin B6 (Pyridoxine) | 50–100 mg | Moderate | Co-enzyme in dopamine/serotonin synthesis; promotes hepatic estrogen clearance | 1–3 cycles | Doses > 200 mg/day risk peripheral neuropathy |
| Magnesium (Glycinate/Citrate) | 300–400 mg | Moderate | Lowers cortisol; regulates FSH/LH pituitary release; supports GABA calm | 2–4 weeks | Citrate form causes loose stools; contraindicated in renal impairment |
| Zinc (Picolinate/Sulfate) | 15–30 mg | Preliminary–Moderate | Drives FSH production; supports follicular development and corpus luteum quality | 1–3 cycles | > 40 mg/day induces copper deficiency |
Also consider: supporting herbs to increase progesterone alongside these nutritional foundations for a comprehensive approach.
Your actionable step: Begin with Magnesium Glycinate 300 mg at bedtime immediately — this addresses both the cortisol suppression and the sleep disruption within days, creating the hormonal conditions for progesterone recovery to follow.
What foods support or harm progesterone levels?
Foods that support progesterone provide the micronutrients essential for corpus luteum function and steroidogenesis: Vitamin C from citrus and bell peppers, Zinc from pumpkin seeds and lean beef, and Magnesium from dark leafy greens and almonds. Foods that harm progesterone include alcohol, excessive caffeine, and conventional non-organic meat containing synthetic hormones.
Because progesterone is synthesized directly from cholesterol, ultra-low-fat diets and severe caloric restriction eliminate the raw biological material required for hormone production. This is why women in extreme exercise or chronic undereating frequently lose their cycles entirely — the body shuts down progesterone production as a survival response.
Caffeine is specifically problematic during the luteal phase: its clearance slows significantly in the two weeks before your period, meaning it accumulates, disrupts estrogen metabolism, and worsens the breast tenderness, anxiety, and sleep disruption that already accompany declining progesterone.

FAQ
What are the first signs of low progesterone?
The earliest signs appear in the luteal phase, the two weeks before menstruation. Brown spotting before your period, cycles shorter than 24 days, sudden sleep onset difficulties, and escalating PMS mood swings are the first signals that the corpus luteum is not producing adequate progesterone after ovulation.
Can you have low progesterone with a regular period?
Yes. Anovulatory cycles produce a period-like bleed from estrogen withdrawal without any ovulation occurring — meaning no corpus luteum forms and no progesterone is produced. Alternatively, ovulation occurs but the corpus luteum peaks too low or collapses too quickly, producing a Luteal Phase Defect with technically regular cycles but severely suboptimal progesterone throughout.
What is the difference between a normal and an optimal progesterone level?
Standard laboratory ranges consider 1.8–24.0 ng/mL normal during the mid-luteal phase. Functional medicine targets 10–25 ng/mL as optimal, because levels between 1.8 and 9.9 ng/mL — technically “normal” — are consistently associated with severe PMS, insomnia, anxiety, early spotting, and elevated miscarriage risk. Your doctor dismissing your labs as normal does not mean you are not experiencing real hormonal suffering.
Does low progesterone cause hair loss?
Yes. Low progesterone reduces the liver’s conversion of inactive T4 into active T3, creating functional hypothyroidism even when standard thyroid tests appear normal. This sluggish thyroid hormone utilization produces the classic triad of fatigue, weight gain, and hair thinning — which is why so many women with low progesterone are incorrectly treated for thyroid disease alone.
How long does it take to raise progesterone naturally?
Clinical data shows that natural interventions — Vitex agnus-castus, Vitamin C, Vitamin B6, and targeted dietary changes — require 90 days (three complete menstrual cycles) to achieve measurable improvement in serum progesterone and sustained symptom relief. This timeline reflects the time required to improve follicular development, corpus luteum quality, and HPA axis regulation. Building healthy hormonal lifestyle habits alongside supplementation accelerates this process.
Can stress alone cause low progesterone?
Yes. Chronic stress elevates cortisol, which signals the hypothalamus to suppress GnRH — the master hormone that initiates the entire ovulatory cascade. Without a GnRH pulse, LH and FSH are not released, follicles do not mature, ovulation does not occur, no corpus luteum forms, and progesterone production drops to negligible adrenal levels. Stress does not steal progesterone; it prevents the body from manufacturing it at all.
When should I see a doctor about low progesterone symptoms?
Seek evaluation if you experience cycles shorter than 21 days, spotting lasting more than 3 days before your period, recurrent miscarriages, severe PMDD symptoms affecting your daily function, or perimenopausal mood symptoms severe enough to disrupt relationships or work. Request a mid-luteal serum progesterone test timed 5–7 days post-ovulation, alongside FSH, LH, estradiol, prolactin, cortisol, TSH, Free T3, and fasting insulin.
Works Cited
- American Society for Reproductive Medicine. “Diagnosis and Treatment of Luteal Phase Deficiency: A Committee Opinion (2021).” ASRM. URL: https://www.asrm.org/practice-guidance/practice-committee-documents/diagnosis-and-treatment-of-luteal-phase-deciency-a-committee-opinion-2021/
- Cleveland Clinic. “Low Progesterone: Causes, Symptoms, Tests & Treatment.” URL: https://my.clevelandclinic.org/health/diseases/24613-low-progesterone
- Cleveland Clinic. “Progesterone: Natural Function, Levels & Side Effects.” URL: https://my.clevelandclinic.org/health/body/24562-progesterone
- NIH StatPearls. “Physiology, Progesterone.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK558960/
- NIH StatPearls. “Progestins.” NCBI Bookshelf. URL: https://www.ncbi.nlm.nih.gov/books/NBK563211/
Increase Progesterone Naturally — What Doctors Miss